Dr. Nikolaos Barotsis presents a case report that demonstrates the successful combination of focused shock wave and radial pressure wave treatment for lateral epicondylitis, commonly known as “tennis elbow.”
Lateral Epicondylitis of the Elbow
Lateral epicondylitis, also referred to as “tennis elbow,” is a prevalent overuse syndrome affecting the upper limb. While it is commonly associated with athletes, it is also frequently observed in non-athletes. The primary cause is tendinopathy of the common extensor tendon (CET), which serves as a partial attachment for the extensor carpi radialis brevis, extensor digitorum, extensor digiti minimi, and extensor carpi ulnaris.
Patients experience pain on the lateral side of the elbow, which worsens with wrist extension, along with tenderness over the lateral epicondyle. Clinical examination is typically sufficient for diagnosis, although ultrasound imaging provides valuable diagnostic information, such as the presence and size of tendon tears frequently observed in tendinopathies. By understanding the etiology and nature of the problem, we can effectively guide treatment and achieve optimal outcomes.

Case Report
A 55-year-old woman had been experiencing lateral elbow pain for several months, particularly when lifting or gripping heavy objects. She reported that the pain worsened two weeks before the examination, following intense household activities, and had remained stable since then.
Clinical examination confirmed the typical signs of lateral epicondylitis. Ultrasound imaging revealed diffuse hypoechogenicity and thickening of the CET at its origin, as well as the presence of an osteophyte and small intratendinous tears (fissures) (Figure 1).
The patient initially received non-steroidal anti-inflammatory drugs (NSAIDs) for one week, followed by a program involving stretching and progressive strengthening exercises for the wrist and finger extensors, along with the use of a forearm counterforce brace.
However, after two weeks, the patient continued to experience severe pain, with no improvement observed during the clinical examination or ultrasound scan (Figure 2).
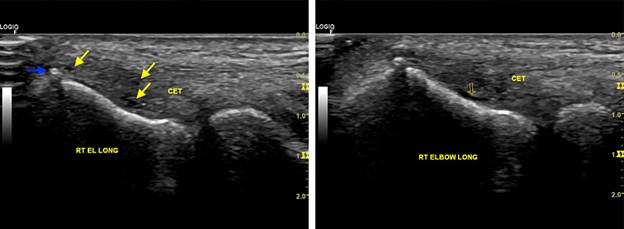
Figure 1: Longitudinal ultrasound image of the right common extensor tendon (CET). The proximal portion of the tendon displays diffuse hypoechoic appearance, thickening, and blurred upper border. Additionally, small intratendinous fissures and calcification are observed. These findings are indicative of lateral epicondylitis of the elbow. Blue arrow: calcification, yellow arrows: intratendinous tears, CET: common extensor tendon, RT EL Long: longitudinal section of the right elbow.
Figure 2: Longitudinal ultrasound image of the right common extensor tendon (CET). Following 2 weeks of conservative treatment involving non-steroidal anti-inflammatory drugs (NSAIDs), exercises, and bracing, the CET continues to exhibit sonographic evidence of tendinopathy and intratendinous tears. Void arrow: intratendinous tear, CET: common extensor tendon, RT ELBOW LONG: longitudinal section of the right elbow.tear, CET: common extensor tendon, RT ELBOW LONG: longitudinal section of the right elbow.
Treatment
The patient received a total of five extracorporeal shock wave therapy (ESWT) sessions with one-week intervals. Before each session, an ultrasound examination was conducted, and the affected area displaying pathological findings was marked on the skin to guide the targeted application of ESWT (see Figure 3, 4). Half of the pulses were focused on the most affected part of the tendon, as indicated by the ultrasound scan, while the remaining pulses were applied to the rest of the common extensor tendon (CET).
In addition, the extensor muscles of the arm and forearm were examined for trigger points using focused shock waves. Shockwave Therapy pulses were administered per trigger point, utilizing the same settings employed during the scanning process. The focused shock wave therapy was targeting muscles with myofascial trigger points (see Figure 5a, 5b). The patient was advised to continue their regular daily activities but to refrain from engaging in sports or exercise until the ESWT sessions were completed.
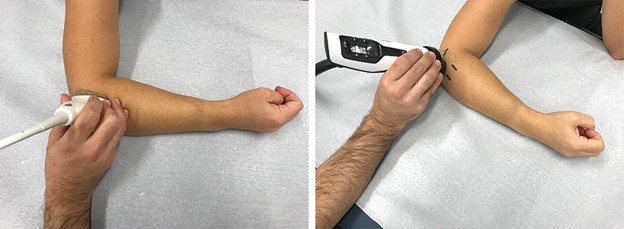
Figure 3: The ultrasound examination of the lateral elbow involved placing the probe longitudinally over the common extensor tendon (CET). In order to facilitate the guidance of extracorporeal shock wave therapy (ESWT), the skin was marked at the location where the ultrasound revealed the most significant pathological findings.
Figure 4: Application of focused ESWT.
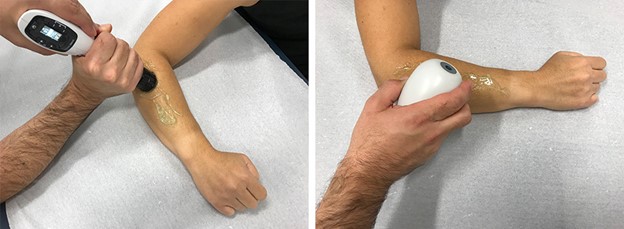
Figure 5a and b: The radial Shock Wave hand piece, equipped with a D20s transmitter, is shown. Myofascial pain syndrome affecting the extensors of the wrist and fingers, as well as the biceps brachii and anterior brachialis, is frequently observed in individuals with chronic lateral epicondylitis of the elbow. By addressing not only the tendinopathy of the common extensor tendon (CET), but also the associated disorders, effective treatment of lateral epicondylitis can be achieved.
Results
The level of pain, as measured on the visual analogue scale (VAS), reduced from 9 prior to the first treatment to 3 by the final session. One month later, the patient experienced complete relief from symptoms. During the ultrasound scan conducted at the last session, milder signs of tendinopathy were observed compared to the initial examination, and the tears were completely healed (see Figure 6).
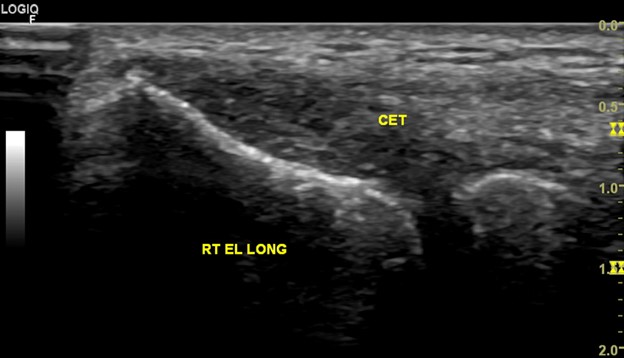
Figure 6: The ultrasound examination conducted during the final session of ESWT revealed notable improvements, even though it was still early to detect changes in the ultrasound findings. The examination showed reduced hypoechogenicity and tendon swelling, as well as a more distinct upper border of the tendon compared to the initial examination. At this stage, the intratendinous tears were completely healed. The restoration of normal echotexture is typically anticipated within six months following the first ESWT session. (CET: common extensor tendon, RT ELBOW LONG: longitudinal section of the right elbow)
Image credits: Dr. Nikolaos Barotsis and STORZ Medical
Dr. Nikolaos Barotsis, MD.
Physiatrist, MSK Ultrasonographer
Senior Fellow of the European PRM Board
Academic Fellow, Rehabilitation Centre, Patras University, Rio – Greece
Vice President of UEMS PRM Board